
Your team is probably in a familiar spot. Engineering is moving fast, the prototype works, investors want timelines, and someone has finally asked the uncomfortable question: what could go wrong when this device reaches a patient, a clinician, or a home user?
That question changes the whole conversation.
In medtech, a promising design isn't enough. A device has to be safe in normal use, safe in foreseeable misuse, and still controlled when manufacturing variation, software changes, servicing, and real-world behavior start exposing the edge cases nobody saw in the demo. That's why risk management of medical devices sits at the center of product development, quality, and market access. It isn't paperwork added at the end. It's the discipline that tells you whether your product is ready to earn trust.
Teams that understand this early usually make better decisions. They define intended use more sharply. They write better requirements. They test the right things. They also avoid the common trap of treating compliance as a final gate, when it should shape design choices from the start.
Why Medical Device Risk Management Matters More Than Ever
A startup team can spend months refining features and still miss the core issue. The burden isn't just proving that a device works. It's proving that foreseeable harm has been identified, evaluated, controlled, and monitored after release.
That distinction becomes painfully clear when teams move from prototype thinking to patient safety thinking. A wearable, monitoring tool, or therapy device may look polished in internal testing, yet fail in ways that only become obvious when users wear it incorrectly, ignore instructions, use it in noisy environments, or update companion software at the wrong time.
The stakes are human and commercial
Risk management of medical devices matters because device failures don't stay inside engineering. They reach patients, clinicians, support teams, insurers, and regulators. They also reach your brand.
An industry summary citing National Library of Medicine data reports that more than 54.5% of device recalls were associated with product design issues that stronger risk management could have prevented or reduced, according to this review of risk management strategies. That should get every founder's attention. More than half of the recall burden in that dataset tied back to upstream design and control decisions.
Practical rule: If a hazard can be discovered earlier through intended-use definition, design review, usability work, or verification planning, find it there. Field discovery is the most expensive place to learn.
A useful way to think about it is this. A recall is rarely just a quality event. It's often the final visible symptom of earlier choices that weren't challenged hard enough.
Good risk work supports better product design
Strong risk practice doesn't slow innovation. It sharpens it. Teams building modern wearables, mobility aids, remote monitoring tools, and solutions for sedentary cardio all face the same underlying reality: the closer a device gets to a user's body, routine, or clinical decision-making, the less room there is for ambiguity about safety controls.
A mature team starts asking better questions:
- Intended use clarity: What exact user, setting, and condition is this device designed for?
- Misuse awareness: How will people use it when instructions are rushed, skipped, or misunderstood?
- Control effectiveness: Which protections are built into the design, and which ones rely too heavily on labeling?
- Post-release discipline: What process catches emerging issues once the device is in the field?
The competitive advantage isn't just fewer surprises. It's a device program that can survive scrutiny.
Understanding the Core Principles of Risk
While the term "risk" is often used loosely, regulators don't. In medical devices, risk has a specific meaning under ISO 14971:2019. The FDA's CDRH training material explains that risk is the combination of the probability of occurrence of harm and the severity of that harm, and it highlights PHA, FTA, and FMEA as common analysis methods in the framework described in this FDA training reference.

Risk isn't the same as failure
A simple street-crossing analogy helps. A moving car is a hazard source. Stepping into traffic at the wrong moment is the hazardous situation. Injury is the harm. Risk comes from combining how likely that harm is with how serious it would be if it happened.
Medical devices work the same way.
A battery overheating isn't automatically the harm. Neither is a software calculation fault. Those are part of the chain. What matters is how that chain can expose a user or patient to a dangerous situation, and what the outcome could be.
The terms that matter in audits
Teams should get comfortable with a few terms because they shape your documentation and design decisions.
| Term | Practical meaning |
|---|---|
| Hazard | A potential source of harm |
| Hazardous situation | Circumstances that expose someone to the hazard |
| Harm | The injury or damage that results |
| Risk | The combination of severity and probability of harm |
This sounds formal, but it improves communication. Instead of saying "the alarm is risky," a stronger statement is: the alarm may fail to activate under a specific condition, which could delay user response and expose the patient to harm.
Clear risk language improves engineering. It forces the team to describe cause, exposure, and outcome instead of relying on vague concern.
ISO 14971 is the shared language
Think of ISO 14971 as the rules of the road. It doesn't design the car for you, but it tells you how to identify hazards, assess consequences, choose controls, and justify what remains.
That matters because cross-functional teams often talk past each other. Engineers focus on failure modes. Clinical staff focus on harm. Quality focuses on traceability. Regulatory focuses on acceptability and evidence. ISO 14971 gives those groups a common structure.
In practice, useful risk conversations ask questions like these:
- What can cause harm in normal use?
- What happens in fault conditions?
- How bad is the outcome if control fails?
- How likely is the path to harm?
- What evidence supports that estimate?
When a team can answer those questions precisely, it's no longer "doing compliance." It's designing responsibly.
The ISO 14971 Lifecycle Explained
Risk management of medical devices works best when treated as a loop, not a binder on a shelf. Under ISO 14971, manufacturers must identify hazards, estimate and evaluate risks, implement and verify controls, and continuously monitor production and post-production information, using objective evidence and pre-defined acceptability criteria in a traceable process described in this ISO 14971 lifecycle overview.

Plan before you score anything
Many teams rush into spreadsheets and start assigning severity and occurrence scores before the foundation exists. That's backwards.
The first discipline is planning. The risk management plan should define intended use, roles, review points, methods, and risk acceptability criteria. If acceptability criteria aren't defined up front, teams end up making residual-risk decisions emotionally or politically. One group calls a risk acceptable because launch pressure is high. Another calls it unacceptable because no one agreed on thresholds in advance.
A solid plan also answers a practical question auditors often expose quickly: who is authorized to decide that residual risk is acceptable, and based on what evidence?
Build the hazard-to-control chain
A workable lifecycle usually follows this chain:
- Identify hazards tied to intended use, foreseeable misuse, environment, interfaces, servicing, and disposal.
- Describe hazardous situations in concrete terms.
- Estimate risk using objective evidence where possible.
- Evaluate acceptability against pre-defined criteria.
- Implement risk controls through design, protective measures, and information for safety.
- Verify control effectiveness so protection is demonstrated, not assumed.
- Review residual risk and decide whether benefit supports release.
- Monitor post-production signals and feed them back into the file.
That chain matters because traceability is where many systems either become defensible or fall apart.
If you can't trace a hazard to a control and then to verification evidence, the control exists only as an intention.
Post-production is where mature systems separate from weak ones
A launch isn't the end of risk work. It's the point where assumptions meet reality.
Production issues, complaint trends, service findings, CAPA activity, software updates, and field observations all belong in the feedback loop. If teams only revisit risk during formal audits or submission preparation, they're managing appearances, not risk.
A practical post-production discipline often includes:
- Complaint review linkage: New complaints are screened for previously unidentified hazards or degraded controls.
- Change impact review: Design, supplier, manufacturing, and software changes trigger risk reassessment.
- Verification refresh: Controls affected by change are rechecked, not merely referenced from old evidence.
- Periodic management review: Leadership sees risk status as an operating issue, not just a quality record.
The best systems keep the file alive. When that happens, the risk record stops being a regulatory artifact and becomes an operating tool for safer decisions.
Practical Risk Analysis Techniques and Examples
FDA materials recommend using multiple complementary techniques, including FMEA for component or process failures and FTA for top-event causation chains, because different methods expose different failure dynamics, as outlined in FDA guidance on risk techniques. That recommendation aligns with what experienced teams already know. One tool rarely sees the whole picture.
FMEA starts at the component level
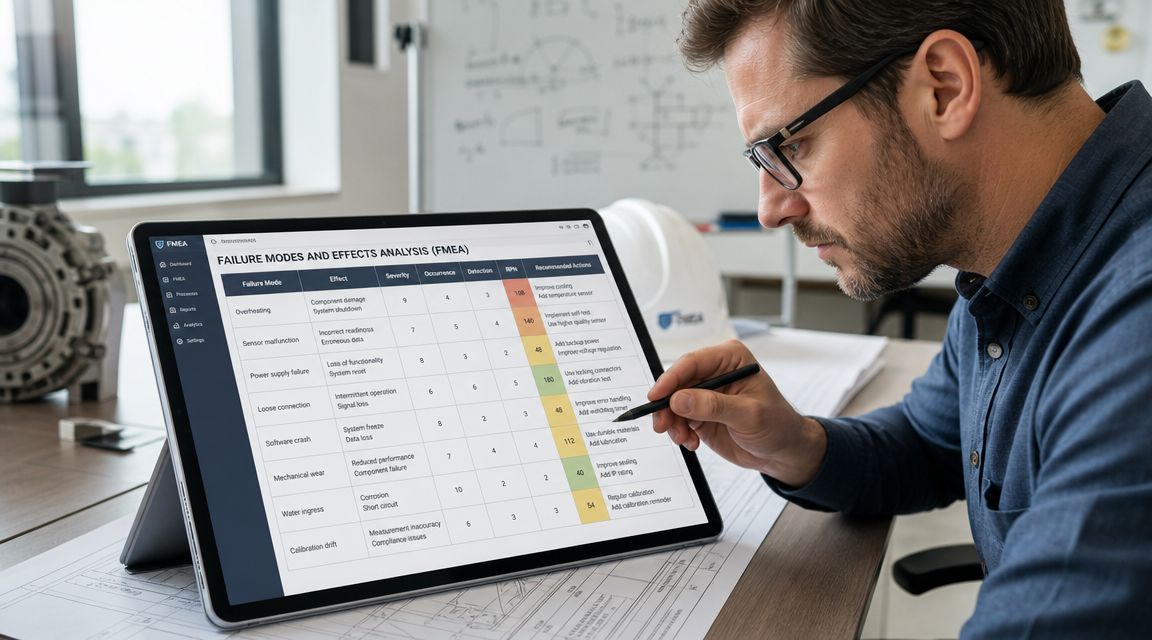
Failure Modes and Effects Analysis is a bottom-up method. You start by asking what happens if a specific part, process step, interface, or software function fails.
Use a coffee maker as a simple example. A heating element may fail to shut off. A temperature sensor may drift. A lid interlock may not engage. Each of those failure modes has an effect, and each effect can lead toward user harm under certain conditions.
FMEA is useful when you need discipline around granular failure thinking, especially in design and process reviews.
A practical FMEA discussion often includes:
- Failure mode: What exactly fails?
- Effect: What happens at subsystem or user level?
- Cause: Why would the failure occur?
- Current controls: What already prevents or detects it?
- Recommended action: What should change in design, process, or verification?
For teams new to structured analysis, external perspectives on maintenance FMEA insights can also help frame how failure logic transfers across operational settings.
FTA starts with the bad outcome
Fault Tree Analysis works in the opposite direction. It is top-down. You begin with a serious event and ask what combinations of failures could cause it.
Take the same coffee maker. Start with the top event: user receives a burn injury. Then work backward. Was there overheating? Did steam vent unexpectedly? Did the handle detach? Did a sensor fail while a backup cutoff also failed? FTA is strong when the team needs to examine causal pathways and interacting conditions rather than isolated component faults.
That's why FTA is often more revealing for system-level hazards, alarms, power events, combined failures, and software logic paths.
When to use which method
The simplest distinction is this:
| Technique | Best for | Thinking direction |
|---|---|---|
| FMEA | Component, subsystem, process, and function failures | Bottom-up |
| FTA | Serious system outcomes and causation chains | Top-down |
Neither method replaces the other. If your team relies only on FMEA, you may miss combinations of events that individually look harmless. If you rely only on FTA, you may miss routine component and process weaknesses that should have been controlled earlier.
The most useful risk files don't just contain analyses. They show why a given method was chosen for a given question.
For broader process framing, this guide to risk analysis for businesses is a helpful operational lens, especially for teams translating abstract risk language into repeatable decision-making.
What doesn't work in practice
Weak teams often make the same mistakes:
- Scoring without context: Numbers get assigned before the hazardous situation is clearly described.
- Label-heavy controls: The file says the risk is controlled by warnings, but the design could have reduced the hazard directly.
- No verification link: The mitigation exists in a row, but nowhere in testing.
- Single-tool dependence: The team assumes one worksheet is the full analysis.
Strong teams use the method to force sharper design decisions. That's the point.
Building Your Risk Management File
The Risk Management File, or RMF, is the auditable record of your device's safety story. It should show what you knew, what you considered, what you decided, what controls you implemented, and how you know those controls work.
Teams often dread this part because they imagine a stack of disconnected templates. In well-run programs, the RMF is not a document dump. It is the structured narrative that connects intended use, hazards, controls, verification, and post-market learning.
Think of the RMF as the device biography
A useful way to explain the RMF to product teams is this: it is the biography of how the device was made safe enough for its intended use. Not perfectly safe. No device is. Controlled, justified, and monitored.
The strongest files make it easy to follow the thread from concern to evidence. A reviewer should be able to see a hazard, understand the hazardous situation, find the selected control, and locate proof that the control was implemented and verified.
What the file usually needs to contain
The exact structure can vary, but a practical RMF typically includes these core elements:
- Risk management plan: Scope, responsibilities, methods, review criteria, and acceptability framework.
- Hazard identification and analysis: Known hazards, sequences of events, hazardous situations, and potential harms.
- Risk evaluations: Clear judgments about which risks are acceptable and which need control.
- Risk control records: Design changes, protective measures, alarms, interlocks, software checks, labeling, and training-related decisions where relevant.
- Verification evidence: Test reports, inspection results, design review outputs, and other proof that controls work as intended.
- Residual-risk assessment: The rationale for remaining risk and, where needed, benefit-risk reasoning.
- Risk management report: A formal summary that concludes whether the process was followed and the device is acceptable for release.
- Production and post-production inputs: Complaints, service information, nonconformities, and change-triggered reassessments.
A thin RMF usually means one of two things. The team either didn't do the work, or it did the work but failed to preserve the evidence.
What auditors and reviewers notice quickly
They notice broken traceability, outdated assumptions, and contradictions between departments. If software changed but the hazard analysis did not, that gap stands out. If a known risk control appears in requirements but not in verification, that stands out too.
A practical RMF habit is to review it at the same time major product decisions are made. When intended use shifts, interfaces change, suppliers change, or software behavior changes, update the file then. Waiting until submission prep turns risk documentation into archaeology.
Integrating Risk Management with Agile and DevOps
Many modern teams struggle to reconcile these diverse approaches. Agile values iteration. DevOps values flow. Medical-device risk management demands deliberation, traceability, and evidence. Teams often assume those worlds conflict. They don't. But they do require discipline.
Modern risk management must extend beyond initial design to cover software, cybersecurity, and AI behavior changes after release, because connected devices need controls that remain effective after patches and data-driven updates, as discussed in this review of evolving medical-device risk practice.

Put risk into the sprint, not after it
A common failure pattern looks like this. The software team ships features sprint by sprint. The quality team performs risk review later. By then, architecture choices are already baked in, and "mitigation" becomes a scramble of warnings, patchwork checks, and retrospective justifications.
A better operating model embeds risk into routine delivery work.
For example, a user story that changes dose calculation logic, alarm behavior, data synchronization, or permissions should trigger explicit risk questions before closure. If your sprint board tracks only functionality, you're missing the safety dimension.
A practical definition of done for regulated software often includes:
- Risk impact assessed: The team decides whether the change affects hazards, hazardous situations, or existing controls.
- Requirements updated: Safety-related behavior is reflected in controlled requirements.
- Verification mapped: Test evidence covers the change and any impacted risk controls.
- Traceability preserved: Design, risk, and verification artifacts stay linked.
- Release decision reviewed: If residual risk changed, the right approvers see it.
CI/CD needs compliance guardrails
Continuous integration is valuable in medtech. Uncontrolled continuous deployment is where trouble starts.
Teams can still move fast if the pipeline enforces checks around code review, test evidence, configuration control, and change impact. The point isn't to slow every commit. It's to make sure safety-relevant changes cannot pass undetected into release candidates.
For software leaders aligning delivery practice with quality expectations, this explainer on continuous integration in modern teams is a useful non-regulatory framing for how disciplined automation supports repeatability.
Software risk doesn't stop at release
Connected devices create a harder problem than traditional hardware. A patch can remove one vulnerability and introduce a timing issue elsewhere. A cloud configuration change can alter device behavior indirectly. An AI-enabled feature can drift from what the original validation assumed if update governance is weak.
That means risk management of medical devices now needs operational controls such as:
- Software change governance: Every update gets a formal impact assessment tied to hazards and controls.
- Cybersecurity-by-design: Security controls are treated as safety-relevant when compromise can affect device behavior or data integrity.
- Field monitoring: Production logs, support issues, complaints, and anomaly signals feed back into risk review.
- Rollback readiness: Teams know how to contain a problematic release without improvising under pressure.
Fast release cycles don't remove the need for evidence. They increase the need for it.
The teams that succeed here don't bolt compliance onto Agile. They redefine Agile work so safety and compliance are native parts of delivery.
Navigating Complexity with a US-Based Outsourcing Partner
For many SMEs, the hardest part isn't understanding the principles. It's sustaining them. Risk management of medical devices takes cross-functional judgment, documentation discipline, software awareness, and regulatory fluency over time. Most smaller organizations don't have deep bench strength in all of those areas.
That's where an outsourcing model can become strategic instead of transactional.
Why US-based support is often the safer choice
A US-based outsourcing partner brings proximity to FDA expectations, stronger alignment with documentation practices common in US submissions, and easier coordination across product, quality, regulatory, and engineering stakeholders. Time zone overlap matters more than teams expect when a design change, field issue, or release decision needs same-day review.
There's also an accountability advantage. In regulated work, ambiguity is expensive. You want a partner that can work directly with your internal owners, document decisions clearly, and support evidence generation without treating risk files as generic admin work.
What a strong partner should actually do
The right partner doesn't just "help with compliance." They should strengthen execution in specific ways:
- Process design: Build or refine a risk process that fits your development workflow instead of fighting it.
- Documentation control: Keep plans, analyses, reports, and traceability current as the product evolves.
- Software-aware review: Assess how updates, integrations, and cybersecurity changes affect residual risk.
- Independent oversight: Provide objective challenge when teams are too close to their own design assumptions.
- Scalable capacity: Add specialist support during design reviews, submission preparation, remediation, or post-market response.
For startups and growing product teams that need flexible operational efficiency, this perspective on outsourcing for scaling across the USA, Canada, and Europe captures the broader business case well.
A key benefit is focus. Your internal team can keep building the product while experienced external support helps keep the safety case coherent, current, and defensible.
If your team needs help building a practical, audit-ready risk program around software, documentation, and ongoing operational control, NineArchs LLC can support the work with scalable outsourcing and technical delivery capacity. For guidance on integrating risk management into your product lifecycle, call (310)800-1398 / (949) 861-1804 or email [email protected].



